
(H/T to Another Ian for pointing at this in a comment.)
Jo Nova has a page up here:
https://joannenova.com.au/2021/07/mexico-uses-ivermectin/
Which looks at the experience in Mexico as they were having a very bad time of it, then, almost in desperation, they rolled out Ivermectin. Their report of deaths immediately turned from a rising spike at the start of the year to a downward plunge. Now actual deaths are below expected deaths. They are having LOWER than “normal” rate of deaths.
Here’s the graph from Jo’s place:
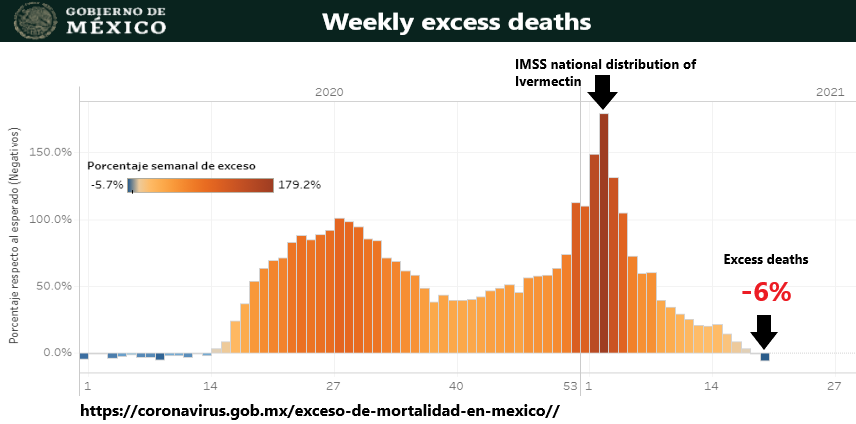
Mexico Starts Ivermectin Use, Deaths turn from Spike to Plunge
From Jo’s article:
For a whole year more people were dying in Mexico than normally died. There’s been one long bloodbath there and an untold story. Mexico may not have hit the “photogenic” headline stage that Brazil, Iran, and India did, but nonetheless, somewhat unnoticed, it’s been continuously bad.
[…]
The wave of 2020 ran for a whole year with deaths running at 50 – 100% higher than in a normal year. Since the pandemic began some 350,000 excess deaths have been recorded. The death toll for Covid in Mexico may be 60% higher than the official Covid casualty count of 230,000. As winter made the situation even worse, things got desperate enough (finally!) for cheap treatments to be organized.Ivermectin use at 200 microgram/kg started on December 21 and was gradually rolled out across Mexico. It took months, but finally, for the first time in a year, Mexican deaths are back to normal, and even slightly lower.
Hit the link for the rest of the article and for links on to other sites and some backup information / evidence.
This is the Official Mexican site from which Jo got the original of that graph. You can click through and see it live with current data.
https://coronavirus.gob.mx/exceso-de-mortalidad-en-mexico/
They make the site particularly difficult for copy / paste of the text, even print to PDF doesn’t capture it, so some exotica (or just retyping it) might be needed.
As an alternative to Google Translate, here’s a Spanish-English translation link:
https://www.translate.com/spanish-english
Just so any non-Spanish speakers can check for themselves what the titles and such say.
In Conclusion
We now have an existence proof (in reality, a few of them in different countries) that use of Ivermectin ENDS Chinese Wuhan Covid as a national threat.
FWIW, I’m also an existence proof of sorts. I’ve been living in the center of one of the earliest hot spots of “community spread” and for over a year I’ve been using Ivermectin while I just went about my life. I’ve also driven coast to coast and been in the middle of a 1/4 million person peaceful protest with just about nobody wearing masks. All with no sickness. I think that counts as a proof of sample size one. (Two, actually, spouse didn’t get sick either, but she didn’t do the road trip).
In my opinion: The only reason NOT to use it, is because you want to continue this sickness. Any politician who is against its use is desiring the deaths, debility and dependency of their citizens. Any company or petty government “official” who is against the use of ivermectin is either “On the take”, making a huge profit, or an incompetent idiot who can not read a graph. (Or all of the above, and “willfully blind”). I suppose there is also a case to be made for psychopathic / sociopathic disordered folks who have moved up from pulling wings off flies and lighting cats on fire to murder by proxy… but that’s hardly an endorsement. /snark;
Not willing to end on such a dour note, the upside:
YOU can take care of yourself and your family. We’ve talked about how to use ivermectin and how to get it a few times. If you are fence sitting, well, now you know what it has done for Mexico. Find an M.D. who will write a prescription and be well.
We also now have a very nice “Tell” for who is truthful and clueful vs. those who are dishonest, pwned, or “useful idiots”. If someone protests the use of Ivermectin, show them this graph. If they persist in being negative about it, you know you need not pay any more attention to them. They are either evil or an unthinking drone with bad information. Mark them “do not believe” and move on.
FWIW, this morning I applied my “once a week” preventative Ivermectin treatment. For 100 kg body mass, 10 ml of “Ivermectin Drench” 5mg ivermectin / ml. Same dose as for sheep. 50 mg total or 0.5mg/kg. Or 500 mcg / kg. Note that this is 2.5 times larger than the dose used in Mexico. As the dose range (“therapeutic range”) for ivermectin is quite large, up to 40 times the minimum dose, I’m willing to accept that a topical dose (the ‘drench’ just soaks in through your skin, it is not swallowed) might need a higher dose for losses in the skin or failure to reach the blood, when compared to oral pills for humans. But it is equally possible that a 4 or 5 ml dose would work just as well.
Several studies used that 200 mcg/kg dose for medical professionals, IIRC, and at an every-other-week dose level there were a few cases. Changed to once a week they had zero cases. I think this was the case in India.
The FLCCC has a few protocols for other uses. This one is for global use in prevention. The target body mass is 40 kg / 90 lbs, so quite low compared to my size:
https://covid19criticalcare.com/covid-19-protocols/i-mass-protocol/
18 mg once per week (along with vit D 2000 IU and a daily multivitamin)
As I’m about 2.5 x that big, I’d need 45 mg, making my 50 mg about right. But I do note that it is likely I could cut it in half and still be OK. Though, since 2500 ml cost me $50 (or 2 ¢/ml or 20 ¢ for a full week treatment…) I don’t see the cost benefit of cutting that back from just under 3 ¢ / day to 1.5 ¢ / day.
Getting the feeling this is an incredibly dirt cheap drug? Yeah, even the poorest places on the planet can STOP COVID NOW. With ivermectin cattle drench; if they so choose.
To say otherwise is just Fear Porn of the worst kind. Killing people for an administrative rule and drug paranoia.
Here is the FLCCC protocol for prevention and early outpatient treatment:
Note it uses the 200 mcg / kg does for prevention, but jumps up optionally to 400 mcg / kg for treatment of outpatients. Also note the use of quercetin (a zinc ionophore) & zinc:
PREVENTION PROTOCOL
lvermectin Prevention for high risk individuals
0.2 mg/kg per dose (take with or after meals) — one dose
today, repeat after 48 hours, then one dose weeklyPost COVID-19 exposure prevention
0.2 mg/kg per dose (take with or after meals) — one dose
today, repeat after 48 hours*
Vitamin D3 1,000–3,000 IU/day
Vitamin C 500–1,000 mg twice a day
Quercetin 250 mg/day
Zinc 30–40 mg/day
Melatonin 6 mg before bedtime (causes drowsiness)EARLY OUTPATIENT PROTOCOL3
lvermectin
0.2–0.4 mg/kg per dose (take with or after meals) — one
dose daily, take for 5 days or until recovered*
Use upper dose range if: 1) in regions with more aggressive variants;
2) treatment started on or after day 5 of symptoms or in pulmonary
phase; or 3) multiple comorbidities/risk factors.
Fluvoxamine4 50 mg twice daily for 10–14 days
Add to ivermectin if: 1) minimal response after 2 days of ivermectin;
2) in regions with more aggressive variants; 3) treatment started on
or after day 5 of symptoms or in pulmonary phase; or 4) numerous
comorbidities/risk factors. Avoid if patient is already on an SSRI.
Nasopharyngeal Steamed essential oil inhalation 3 times a day (e.g. VapoRub)
Sanitation and/or chlorhexidine/benzydamine mouthwash gargles and
Betadine nasal spray 2–3 times a day
Vitamin D3 4,000 IU/day
Vitamin C 500–1,000 mg twice a day
Quercetin 250 mg twice a day
Zinc 100 mg/day
Melatonin 10 mg before bedtime (causes drowsiness)
Aspirin 325 mg/day (unless contraindicated)
Pulse Oximeter Monitoring of oxygen saturation is recommended
(for instructions please see page 2 of this file)
[…]
Other languages available at this link:
https://covid19criticalcare.com/covid-19-protocols/i-mask-plus-protocol/
Be not afraid, be pro-active.
Obligatory Lawyer & Petty Bureaucrat Repellent:
I am NOT an M.D. nor do I play one on the internet.
Do NOT consider any of this medical advice. I’m stating my political opinion about treatments, not prescribing anything to anyone.
Always ask YOUR Medical Doctor about what to do for you. You do you. (I’ll do me.)
I might be a flaming idiot who is clueless, so never take any advice from an internet blog. Heck, I might even be a dog at a keyboard for all you know. Or a random bot on a Russian Computer.

On the internet, nobody knows you are a dog.

One of the “this is political” tells is that the search for effective therapeutics using currently available medications was so thoroughly discouraged. Again, in the old days, any sane pharmaceutical company would have immediately tried to find new uses for old drugs, to either get a patent or extend one. I have to wonder if the vaccine manufacturers were “bought off” long ago via the “legal immunity” laws. I understand why they took it. “Tort” sharks, erm, lawyers were and still are able to “win” big judgments via “emotion”, instead of showing good data as evidence.
EMSmith says; “I might be a flaming idiot who is clueless, so never take any advice from an internet blog. Heck, I might even be a dog at a keyboard for all you know. Or a random bot on a Russian Computer.”
Hell ! I have personally measured the man twice, LOL I certify that He is real and honest to a fault. …pg
Antony Fauci on the other hand seems to be unable to tell the truth about anything. His only consistency is being inconstant and will change his story from day to day as needed.
This drum beat to prevent effective treatments in favor of Emergency Powers to circumvent legal protections of rights should be considered as “Crime Against Humanity”
As for me and mine, we reject their “Jab” and will continue to live our lives as we have for nearly 80 years. and look after our own health…pg
@cdquarls; In early 2019 Bill Gates Bragged in a meeting with investors, that the inoculation business model was the best , For every $1 invested $20 was the return!. This about the same time that members of the Gates Foundation was seen (and photographed) touring the Wuhan Lab with Antony Fauci …pg
I had settled on 10 ml Ivermectin every two weeks. I’m now just about to make the switch to 5 ml weekly. That’s my preventative plan dose.
Some months earlier, we discussed how India(?) was giving a monthly dose, but the effectiveness seemed to be 2 to 3 weeks as the Ivermectin was slowly cleared out of the body. I think keeping Ivermectin level instead of a spike and slow drop might be the better strategy.
I did my 10 ml this past weekend. Instead of skipping next weekend, I’m going to start the 5 ml weekly regimen.
Reminder: 1 measuring teaspoon is 5 ml. No need to chase down anything marked in ml. And if you have a 5 ml measuring spoon for cooking, you’re golden 😜
@P.G.:
Yeah, OK, and several other folks saw me over Beer in Clermont Florida… so I guess I can admit that I am, in fact, not a dog ;-)
@H.R.:
I did a posting some time back on dose rate. IIRC the half time was 16 hours so you reached effectively zero blood level at about day 12. Not enough for a 2 week interval and way not long enough for a once / month treatment schedule.
Once a week means you have a fairly steady blood level as the next dose arrives. FLCCC has gone to 1 / week also.
I’m presently using the 10 ml / 100 kg, but the spouse had dropped to the 5 ml dose (she doesn’t like the stuff simply because it smell like rubbing alcohol – the major component – and ‘leaves something on her skin’; i.e. the medicine proper takes a couple of hours to soak in…)
As she has had no issues in several weeks, I probably ought to stop being lazy and swap over to 5 ml also. (Lazy in that the little cattle pour bottle I have has the lowest mark at 10 ml, so I’d have to use some other measure than the bottle. Spouse uses a “graduated shot glass” I got for cooking that has single ml marking on it, so it already is sitting next to the jug…)
But yeah, stuff works even after several 1/2 lives into the end of a week and then some. My use of 10 ml vs 5 ml is all of about 16 hours of the doubled dose… and extending the minimum usable tail out 16 hours. So 12 3/4 days instead of 12…
I suppose one could work out the absolute lower bound working blood level and go to a daily dose method to really stretch the stuff…. 7 x 24 = 168 168 / 16 = 10.5 doublings of the minimum dose. Call it 10. 2^10 = 1024. So, IN THEORY and assuming there’s no bolus kills anything that prophylaxis missed (a huge potential AwShit), 5000/1000 = 5 microliters / day every day. Call it 10 microliters just to be sure. So 0.01 ml. I’m not sure how a normal human could measure that low… I think I’ll stick with the “Bolus and coast” instead of optimal low cost method ;-)
@E.M. – Yeah, that’s the post and discussion I’m remembering.
I figure if I get a snootful of the virus, I’ll jump back up to a heavy 10 ml; splash on s smidge extra. It won’t hurt.
The WuFLu was a 2fer. One was to get Trump out of office. THe other was to start cutting the population down to Ehrlich levels. Hence why Fake-Faucci is still crying wolf.
I think that the Roll-A-Coaster ride might be the best method for your body. The Ivermectin interferes with RNA replication so a period of little or no activity might be best for your long term health.
The bottom line is you want a mild infection for long term immunity to later infections rather then no immunity until Oh shit and you get very sick. Unlike the Fauci shot that offers no immunity just enhanced reactions that may well be worse then the diease,
“They (Mexico) are having LOWER than “normal” rate of deaths.”
Ivermectin is a broad-action agent. A cluster bomb, not a 223. Makes sense.
Easy for a “normal human” to measure sub-milliliter doses:
https://www.hamiltoncompany.com/laboratory-products/syringes/general-syringes/microliter-syringes
Cases and deaths in Mexico began rising again a few weeks ago. Perhaps this is due to abandonment of Ivermectin in some locales. Don’t know why they would do that if it was successful. The deaths chart looks unnatural with abrupt spikes since June.
https://www.worldometers.info/coronavirus/country/mexico/
Scissor: “Don’t know why they would do that if it was successful.”
Skimming, corruption, distribution screw-ups, failure to educate that the use must be ongoing, and cost are all possibilities.
In Mexico, it may not be a matter that their version of a National Health Service has discontinued the plan to give it out. It may be just good ol’ corruption where some local heavy snagged the supply to give to supporters and sell the rest at a higher price to the of the people. And perhaps the price is such that the rest of the ones can’t always afford it.
And IIRC, the initial handout was at a reduced dosage and they still had good results. So they just may be having problems getting more of the kits (or however it was distributed) out to the people.
I don’t know if we have a regular reader here with boots on the ground in Mexico who can give us the real story.
Obviously I’m just guessing at all the possibilities other than a strange decision to stop using Ivermectin. Perhaps the answer will pop up in the next few days or so.
One of the keys to their succes was that one state was already using it with good results and they were using Track & Treat with Ivermectin instead of Track & Trace with Isolation.
Mexico City used the same technique as a study and the results were brilliant
Education in it’s use is obviously important as well.
The COVID data on Mexico’s web site is 7 weeks behind, the last week reported was week 20.
There’s a lot of stuff with Covid that really doesn’t make sense from a scientific point of view. That starts with “patient zero”, which as far as I can tell was in October 2019 when a military Games in Wuhan was held and some French athletes who went caught a very nasty flu-like disease, thus it was circulating in Wuhan by that time. I did link that report (in French) some time ago – it was actually in the news. I’ve also seen reports that when first seen this coronavirus was exceptional for its genetic purity, since normally when a naturally-evolved virus is sequenced there will be a range of mutations. The data on the research at Wuhan was wiped, thus making it impossible to prove that Wuhan was the source but also making that a pretty good bet, since you don’t wipe evidence that would show innocence but only evidence that would show guilt. The NIH research on SARS in 2005 (signed off by Fauci, among others) showed Chloroquine as being effective against that virus (SARS-Cov), and would thus imply that it ought to be effective against SARS-Cov2 to impede replication (thus useful as prophylactic or in early stage of symptoms, not useful later on).
Implications: it’s pretty certain that the virus was a result of gain-of-function research in Wuhan, and probably escaped accidentally. Fauci and Daszak (sp?) were involved in financing this research, and it was done in Wuhan because it was considered too dangerous to be done in the USA. HCQ has fewer side-effects than Chloroquine (which is itself safer than Quinine) and should have been a candidate for RCTs because the research had already been done for SARS-Cov and SARS-Cov2 uses the same ways to invade the cell to replicate.
Hypothesis: the cover-up was done to try to avoid being held responsible, so the CCP, Fauci, and anyone else involved, conspired to bury the evidence. I still don’t see why HCQ was demonised using trials that had too high a dose, too late in the progress (after hospitalisation and intubation), and not including Zinc. Doesn’t make sense at all. About the only idea that seems to hold water here is that the presence of an effective drug would make it illegal to give an Emergency Use Authorisation for the vaccines, but then they also plugged Remdesivir as an effective drug even though it’s pretty ineffective at reducing deaths. Still, that blocking of HCQ implies a much wider conspiracy, with far more doctors involved (or was it the managers who specified the trial conditions because they were told to do things that way?).
Much the same with the demonisation of Ivermectin. It doesn’t make sense scientifically. True that it won’t stop infection, but it does impede replication and thus gives your immune system enough time to gear up to destroy the virus, and that’s what’s really needed anyway – whatever route you take it’s the body’s immune system that actually does the work of destroying the virus.
Meantime, we know that the vaccines don’t stop people catching the virus or becoming infectious and passing it on. My father-in-law (almost 86 now) has had his two shots of vaccine with the second shot around a month ago (probably Pfizer, but the type used is hidden here), but nevertheless got ill with fever and difficulty breathing for a few days around 4 days ago now. He’d had to travel outside the area to get his car repaired, and was talking to someone while it was done, and that appears to be the only possible infection event. He says he’s OK now, but for a time things were somewhat uncertain. I noticed a day or so of that tickle in the throat subsequently, but it went away – seems that illness I had in March was Covid and so my immune system is primed and worked OK, and also implies my FIL was infectious.
Data from countries that have used HCQ or Ivermectin implies a much-reduced death rate. The Swiss data was even more impressive, when their death-rate increased when they banned HCQ for 3 weeks and then removed the injunction against using it, when their death-rate went down again.
Risky for a doctor to prescribe IVM or HCQ here – they can be struck off. IVM (or Stromectol) is no longer easily available either.
I know that people can get stuck with a belief and will stick to it no matter what the data says. Is that the reason for ignoring IVM, or is it something else? I don’t know. It does end up looking like a conspiracy, though.
@Simon:
I see 2 “reasonable” scenarios for why treatments were demonized. Both are corruption.
1) Noble Cause Corruption. There are folks in the medical profession who just know vaccination is the best thing ever. So to promote more vaccine use, they decide that making a (in their view) marginal treatment look like a failure, they are doing God’s Work of advancing the vaccination program. This may interact with the next cause in that they may be sought out and funded by others with a more monetary interest…
2) Greed / Monetary Corruption. There are $Billions to be made out of the vaccinations. Faucci is on the patents. Lots and Lots of money available to fund “studies” to produce a desired outcome, and “grease the wheels” to massive vaccination programs. Merck, for example, disses Ivermectin even though it is the maker just because you don’t get much profit off a 2 ¢ dose… where a $30 vaccine is just great… The Drug Industry is known for manufacturing “studies” to benefit their products. It is also known that paying bribes for results happens. Also just offering to pull all those $Millions of advertising dollars if a media outlet does not get on board can shift Editorial Policy…
There is also some potential for “stupidity”, but these are folks with advanced degrees who are not supposed to be that stupid… so I find this an “unreasonable” reason.
3) Stupidity. It is a remote possibility that the M.D.s doing the studies didn’t understand the drug at all and didn’t think at all about replication. They had very sick patients in the hospital and just wanted to see if this “magic pill” would fix them, so out of stupidity gave it to people without addressing things like Zinc and Vit-D levels, and didn’t understand the cytokine storm came when replication was ending and your immune system was breaking up viruses and spreading their spike proteins all over your body.
My opinion is that it is an interaction of group 1 and group 2 people. That’s where I’ve seen evidence in the media. Note that I’m carefully avoiding the Grand Conspiracy possibility. That there is a Globalist Cabal working hard across many industries and countries to create and promote this disaster for their own Global Domination goals. While there is plenty of evidence for that (in their own words, “Agenda XX”, and deeds), Occam’s Razor favors the “1+2” simpler case.
Worldometer points to this as the source for the current Mexico data:
Click to access Comunicado_Tecnico_Diario_COVID-19_2021.07.06.pdf
from here:
https://www.worldometers.info/coronavirus/#news
EMS – I was on Mexico’s home page.
And remember this, for it is crucial; epidemic season for corona viruses in the tropics and subtropics is *summer*, not winter. That graph is not as useful as it could be, given that the reported numbers are grossly contaminated and misleading. (Just because it is recorded and reported doesn’t necessarily make it be true. Conversely, just because it isn’t recorded and reported doesn’t necessarily make it be false.)
EM – agreed #1 and #2 are the reasonable explanations, but I’m also wondering about the unreasonable one of the CCP adding a bit more weight against the cheaper and less-damaging solutions such as IVM as part of their push towards world dominance. I see much the same when it comes to CAGW, with noble cause corruption and profit being the reasonable explanations but maybe China (or other players such as Soros) adding pressure where needed as a way of destroying their enemy without fighting.
The downside of using IVM treatment in a widespread way looks really minor – it was available as headlice treatment without prescription for use on kids as often as needed. Even if it only reduced deaths/illness by 5% the cost/benefit ratio would be worth it, yet it appears to be better than 80%. A similar lack of any obvious downside if the connection with vitamin D status was publicised and people were made aware of the need to supplement if they don’t spend enough time in the sun for their skin colour. Instead, the lockdowns force people to stay indoors and get even less sun exposure than normal. The obvious increased danger to people with darker skins is presented as being a disparity in medical care (thus racist) rather than being a simple medical fact of deficiency of natural vitamin D.
Once is unfortunate, twice is coincidence, and three times is enemy action…. It does appear that the decisions taken have resulted in far more damage than necessary. It also seems that journals like the Lancet published hit-pieces on HCQ with only a quiet retraction when the data was shown to be unfounded. Maybe they believe that vaccination is the only way, but if so why push an antiviral such as Remdesivir? If they are complaining that the side effects and unknowns with IVM and HCQ are too dangerous, surely the side-effects of the vaccines are also largely unknown – we know some bad side-effects right now (clotting, myocarditis, and deaths), but we can’t know the long-term effects.
Another useful source for Covid information and links is https://www.lenr-forum.com/forum/thread/6222-covid-19-news/?action=lastPost where you’ll find user FM1 puts up a lot of links and extracts that are useful. You’ll soon find who is worth listening to….
Overall, though noble corruption and money ought to be sufficient explanations, I have the nagging feeling that that’s not all that’s happening and that some entities are also helping along their dreams of a global collapse and thus a one-world government springing up. With them governing of course….
@cdquarles re official reporting on cases and deaths:
The data are so skewed and screwed up, particularly for the U.S., that I only consider some other countries’ data as being fairly reliable.
For example I trust Mexico’s reporting and think it’s pretty solid. As best I know, there’s no cheese for their bureauc[rats] so they are not fudging numbers and trying to get an accurate picture. Maybe there are some errors and stumbles, but it is largely correct, IMO.
I cannot trust U.S. Covid reporting. I don’t think it can be ‘fixed’ after being so jiggered up right from the start. You can’t put that toothpaste back in the tube.
.
.
I do trust U.S. hospital admissions data, though. I watch it for rises or declines. The ‘Covid Admission’ numbers are suspect, but the raw total is a decent indicator whether or not to panic.
HR,consider looking at Worldometer and at Mexico’s death graphic. Mexico’s chart remind me of India, in that it is smooth, even the 3 day and seven day averages. ( not like the USA)
Suddenly in Mexico inJune there is a rapid jump in deaths, and a quick and holding or leveling off at a now steady higher death. Yet the cases graphic is a smoothed sweep up from the bottom. The bottom is only a few days before the death chart took off and steadied. None of it looks right to the earlier chart, or other nations charts. Deaths are however holding at a steady rate. I am curious if accounting was changed.
@H. R.,
Without knowing more specifics, I don’t and can’t trust *any* national government’s medical data reports. Definitions matter and those vary from government to government, even within a nation; let alone between national governments. (Hint, does any nation’s infant mortality statistics include therapeutic abortions? /rhetorical)
As David A says, in Mexico and for the southernmost US states, *now* is the time we’d expect to see true case numbers increase, whether death and/or hospitalization numbers do or don’t. What is troubling is the *autumn* numbers for last year and the winter numbers for tropical and subtropical nations plus the corresponding areas of the USA, that is, 35N and southward to 23N).
Oh, another thing: government bureaucracies exist to make the current government look good, whether that’s true or not; and to make political opponents look bad, whether that’s true or not.
Where does incinerating ants with a magnifying glass rank on the psychopathic / sociopathic meter.
Inquiring mind wants know.
@u.k.(us) – It depends on if you’re still doing it in your 20s, 30, 40s, and up.
I burned my last ant when I was in my mid single digit years. They were fire ants, BTW and I was really mad.
.
.
.
.
@David A (and cdq) – Yeah, the way they changed the recording criteria and the changes in accounting rules in the US is one reason I say the ball of twine can’t be untangled. There were several changes that were, near as I can make out, only done to support a particular political narrative.
As cdquarles points out, other countries have made some changes, and they operated using different definitions. I happen to think that a lot of the other countries made fewer changes to reporting procedures and their definitions than the whipsawing we got from our CDC, so I think I get a better picture from the other countries.
Also, different countries tried different approaches to treatments and prevention/containment, so there is some use in comparing other countries.
I just haven’t looked at the U.S. data since last year because I know it’s just presented to support a narrative.
@u.k.(us):
It’s a 3…
;-)
HR, I agree, but the sudden aberration in the Mexico death chart beginning in June does not look right to any chart I have seen. Normally deaths follow a rise in cases with about a two week delay. The Mexico death chart does a sudden spike about five days after a gradual rise, and then quickly levels, while the case count goes up. Also the Mexico death chart is much more variable then any prior time. Unfortunately I have seen no numbers of how many people received and are receiving Ivermectin in Mexico, or the areas of rise. In India there is a very strong correlation to where Ivermectin was and is used, and where it was used and discontinued. Likewise in areas of Africa. I have seen zero instances of correct widespread Ivermectin usage and cases and deaths growing.
Clairification… The Mexico death chart rise is sudden short and quickly levels off. The Mexico case rise is slow and gradual like most. The “gradual “ in my post refers to cases.
Sorry for the sloppy writing.
@David A – It must be a change or delay in recording.
I remember one chart switched from daily cases to a weekly sum and everyone wondered why cases suddenly flattened about 3 or 4 days after the change. Then the week ending sum was posted. Mystery solved.
I think you must view this Stew Peters show: to get a grasp on what is in the “Jab”;
https://rumble.com/vjk0u1-breaking-astrazeneca-vaccine-vials-examined-by-researchers-confirm-toxic-po.html
pay close attention to the information presented at at the end for a hint at the real reason for the multi-Jab program…pg
@P.G.:
Well I watched it to the end, but don’t know what “hint” I was supposed to pick up… Airline pilots having issues?
FWIW, the Graphene Oxide thing was peculiar. It’s not a substance I would want in me (sheet of graphite oxidized with formation of epoxy bonds and more exotica). Yet there is this:
https://pubmed.ncbi.nlm.nih.gov/26814441/
I note with curiosity that ALL the authors have Chinese names… so why is it American vaccines?
“Adjuvants” are junk added to the basic vaccine to antagonize your immune system into a stronger response. They typically are very “not good” for children and other living things… The theory is that the amount of a toxic adjuvant is so low as to not be an important problem. With kids getting up to somewhere around 50 vaccinations, and many of these things being cumulative toxins, I’m not so sure that safety assumption is true anymore.
But what might be the risks?
A random set of links from a search on “graphene oxide blood clots” includes many claims that it causes various blood clotting problems. (Oh, and sidebar, many folks react badly to PEG too).
https://truthcomestolight.com/on-the-connection-between-graphene-oxide-found-in-covid-vaccines-electromagnetic-fields-blood-clots-severe-covid-symptoms-how-to-remove-graphene-oxide-from-the-body/
Valid? Who knows…
But it does look like a chemical I’d not want injected into my blood.
https://en.wikipedia.org/wiki/Graphite_oxide
again in Mexico this week. J Chamie says ‘…the war isn’t over in Mexico Not a surprise that a new surge is growing from Quintana Roo (bottom right in the map)) where a group of MDs are actively blocking IVM treatments. https://facebook.com/COVIDQRoo/posts/no-a-la-ivermectina/283548253281495/ h/t TIP
From Jo Nova site.
@ENSmith; considering the size and shape of this graphene and the fact that it acts as an oxidizer in the cells when broken, What would happen when exposed to extended 5G radiation? Specially after several shots of this substance to accumulate a larger amount in the body.
Everything we are seeing is to get as much of the population as possible to accept on going “booster” shots. Add to this a roll out of 5G everywhere, The shots seem to be randomized as to batch contents as a part this grand experiment that does not confer immunity. Everything about this makes me smell a rat!
The truth is out there if we can make out the pieces…pg
“Vaccines, not the magic bullet the advertisers claim”
https://joannenova.com.au/2021/07/vaccines-not-the-magic-bullet-the-advertisers-claim/
David A: “[…] where a group of MDs are actively blocking IVM treatments.”
I do believe that explains the spike. Nothing to do with delayed reporting or a change in reporting criteria.
Three mutations in the Epsilon coronavirus spike protein dampen the neutralizing potency of antibodies induced by current vaccines or past COVID infections.
The mutations give this coronavirus variant of concern a means to totally evade specific monoclonal antibodies used in clinics and reduce the effectiveness of antibodies from the plasma of vaccinated people.
https://www.sciencedaily.com/releases/2021/07/210706093857.htm
This just occurred to me. It seems there is no reason ivermectin would not work against other viral infections, seeing as it seems to act as a kind of blood conditioner making your blood an unsuitable environment for parasites and viruses seeking to replicate. If it worked against flu viruses, would it not cost the vaccine companies billions quite outside their ivermectin income?
Well, one thing appears certain, vaccinated or not, have IVM at the ready!
Here’s something you guys will love /sarc
Moderna testing mRNA flu vaccine in clinical trial
https://www.foxnews.com/health/moderna-mrna-flu-vaccine-clinical-trial
@P.G.:
Hmmm…. Hadn’t considered that. The molecular shape is rather like some kinds of Fractal Antennas (and BTW that is why a chunk of chicken wire fencing made such good antennas and nobody could explain why – back in the ’70s and before).
5 G has very short wavelength, and fractal antennas can be very small relative to wavelength (due to the multiple paths through the mesh). Might actually couple… Needs some math on sizes, path lenghts and such (or just inject a rodent and toss them in the microwave ;-)
@Rhoda:
IVM is known to work against other viruses including the flu. It is broad spectrum.
@Jim2:
Florida Friend took the jab while on IVM. Had little side effects at all (compared to other folks). Probably because IVM binds to the binding site at the end of the spike protein (picture in some earlier posting about it showing atoms, charges, ionic bonding sites).
IFF I am ever forced to take the jab, it will be one day after a full dose Ivermectin treatment.
I do not take the flu vaccine. (Well, I did ONCE when working at Disney. It was ‘free’ and the spouse was expected to take it in her guest facing role, so I went with here… ZERO reaction on my part as “I’m like that” ;-) I figure that having survived the 1957 Really Bad Pandemic (not as bad as Spanish flu but worse than anything since) my immunity to flu has been very high ever since…
I will certainly NOT take any mRNA flu vaccine. Not for a few years as we see what happens with this first Global Experimental Batch. (Hey, somebody needs to be the control group ;-)
I assume a computer program can simulate mutations of the COVID spike protein, composed of 3831 base pairs, and with pretty good accuracy determine if the resulting protein would bind to ACE2 receptor. This isn’t as complicated as climate and chemical modelling has come a long way, so I think the above would be doable.
Once all the mutations are known and vetted for receptor binding, and of course the number of generations of mutations probably would have to be limited, then create a mRNA vaccine using all the “active” spike templates. That would cover the current spike and potentially many future ones.
Living on 7and 7’s has protected me so far, now all I need is a grant to keep the experiment going.
@u.k.(us): “7and 7’s”?
@Jim2:
There’s a distributed computing protein folding program out there, so yes, you can start a BOINC project and recruit millions of computers as you like it and as their interest vests:
https://boinc.bakerlab.org/
https://unraid.net/blog/help-take-the-fight-to-covid-19-with-boinc-or-folding-home
No code to write, just some molecule layouts to sketch out. (Take present published structure. Make changes. Run them.)
Perhaps this:
https://www.thespruceeats.com/seven-and-seven-cocktail-recipe-761496
HR, something is still goofy on the W-meter chart the large jump in deaths is a one day jump after a steady decline. It occurs near the very bottom of deaths, and it occurs near the very bottom of cases. It makes a one day jump, and then holds stead at that level. Vet strange.
What might be called “Going well – in an unplanned manner”
https://www.infowars.com/posts/epic-memes-bash-bidens-door-to-door-vaccine-task-force/
Probably not the best strategy in the long run.
Pingback: Weekend Links, 10-11 July, 2021 – EZFKA
In keeping with a recent comment that
“If it looks like a duck, walks like a duck and quacks like a duck the fact checkers will tell you it is a squirrel”
Some more “truth serum” for you
“Wokeapedia. How the sausage gets made at the fake information site Wikipedia.”
https://pbs.twimg.com/media/E5sz1L4UcAQSLh7?format=png&name=small
Via http://www.smalldeadanimals.com/2021/07/08/social-disease-86/
@All:
That “pingback” link to “Weekend Links” has a posting just chock full of wonderful memes ;-)
On my little ARM computer, many didn’t load so I had to “right click – pick load image”, so if you get the “broken painting” image not loaded icon, it’s there and it works, but needs a little kick…
@EM: The 7 & 7
Ingredients
1.5 oz. Seagram’s 7 Crown Blended Whiskey
5 oz. 7UP®
Slice of lime
Trial Site News had a YT video “Dr. Robert Malone, Inventor of mRNA technology discusses the Spike Protein”. YT took it down last night. It was an hour long so I had not watched it yet. Now I have found a non-YT source:
https://odysee.com/@Jadu200:7/Dr.-Robert-Malone,-Inventor-of-mRNA-technology-discusses-the-Spike-Protein-_-Int_Full-HD_60fps:2
The mRNA vaccines work by having your own body replicate the spike proteins. There is another vaccine (NovaVax) which uses moth cells to replicate the modified spike proteins. That sounds safer to me, a bit anyway. And the Sputnik V vaccine looks promising https://www.nature.com/articles/d41586-021-01813-2 The current vaccines are at the DOS 1.0 level. And we know that DOS 2.0 was not the final word.
Because of that censored video I looked at the YT “community guidelines” page
https://support.google.com/youtube/answer/9891785?hl=en&ref_topic=9282436
It is long, what you cannot say (or tomorrow, even think).
Content that recommends use of Ivermectin or Hydroxychloroquine for the treatment of COVID-19
Claims that Ivermectin or Hydroxychloroquine are effective treatments for COVID-19
Content that recommends use of Ivermectin or Hydroxychloroquine for the prevention of COVID-19
YouTube doesn’t allow content that spreads medical misinformation that contradicts local health authorities’ or the World Health Organization’s (WHO) medical information about COVID-19.
IVM is safer, but you are not allowed to say that on social media and the MSM will not say that.
Here’s a good article on how the COVID-19 spike was “deactivated” so it couldn’t undergo the change in shape necessary to bind to and enter cells.
Viruses multiply by dumping their genes into our cells and hijacking our cellular machinery to crank out new virus particles. But first, they need a doorway into our cells. Coronaviruses are studded with spikes, which grab hold of proteins decorating our own cells like doorknobs. Once attached, the spike undergoes a dramatic transformation, stretching before partially turning inside out to forcefully fuse with our cells.
Scientists believe that for COVID-19 vaccines to be effective, our immune systems must develop antibodies that prevent this fusion. Such antibodies must target the spike protein in its aptly named prefusion conformation. Unfortunately for vaccine developers, spike proteins are liable to spring from their stubby prefusion shape into their elongated postfusion form on a hair trigger.
Fortuitously, Graham and a former postdoc, Jason McLellan, devised a solution to this problem before the pandemic. Through a bit of structural biology and persistent protein engineering, McLellan discovered that adding two prolines—the most rigid of the 20 amino acids—to a key joint of a vaccine’s spike protein could stabilize the structure’s prefusion shape. This 2P mutation worked in preclinical studies of Graham and Moderna’s MERS vaccine, so they applied it to Moderna’s COVID-19 vaccine.
It also discusses what happens when vaccines make the disease worse.
Although infants who got the vaccine developed antibodies against the virus, they were not protected from infection. Instead, the vaccine seemed to make the disease worse. Some 80% of infants who got the shot were hospitalized after an RSV infection, compared with 5% of infants in the control group. Two vaccinated babies died from the infection. The tragedy tainted the RSV vaccine field for decades.
https://cen.acs.org/pharmaceuticals/vaccines/tiny-tweak-behind-COVID-19/98/i38
I’m a C0VlD survivor (no complications), and a few days after infection, I purchased my equine apple-flavored Ivermectin gel from Tractor Supply ($3.49 plus tax). It tastes as much like apple as a 9V battery tastes like chocolate. Seriously, it’s like taking a 1/4 teaspoon of vaseline.
HiFast – funny! But sounds like not pleasant. At least you didn’t have to take very much.
World Ivermectin Day — July 24
@HiFast – I bought the apple flavored paste ‘just in case’, but I was doing quinine, zinc, and D3 so I never had to go to the Ivermectin.
I finally got the liquid form and am using that as preventative instead of the quinine.
Sounds to me that the paste mixed about 2:1 Peanut butter/paste would probably go down OK.
@ All the paste eaters- No need to choke it down. The same amount rubbed on the skin goes right on in. It is absorbed transdermally.
Not a doctor, don’t take my advice.
I posted this on the Wood thread, but it realy belongs here.
https://www.bitchute.com/video/xWNF3dKU0kP5/
The real history and origins of COVID19.
If you should be so lucky as to have found some IVM pills, it is recommended that you take them with a meal, so the fats in the meal take them into the body, if you are targeting covid. If you are targeting some bug in your stomach, you take them on an empty stomach. According to trusted sources. I have not seen anything that compares the effectiveness of taking it orally or topically. Goebbels [Google and YouTube] censors everything except party line propaganda, so it’s hard to know for sure.
source: comment by johnhenryb to
https://trialsitenews.com/authoritarian-rise-youtube-targeting-trialsite-and-cutting-several-news-rundown-episodes/
As an example of how intelligent people work (including some scientists), Bret Weinstein has a video which lists the arguments against taking IVM. Not because he is against it, he is not, but as an example of a steel-man argument as opposed to a straw-man argument.
Will Goebbels take this one down too? If so it is also on his Odysee channel
https://odysee.com/@BretWeinstein:f/EvoLens84:b
And in case you want to know what a steel-man argument is:
https://constantrenewal.com/steel-man/
“The Steel Man Technique: How To Argue Better And Be More Persuasive”
YouTube is Evil. They have taken down more Dr. Been videos which mention IVM.
He is going to put his videos on Odysee too.
This new one is good if you like to see the details about how something works.
In this case, the vaccines produce antibodies against the spike protein, but those antibodies also attach to Platelet Factor 4 (in some people), causing clotting.
Here’s an article on the “platelet 4” issue.
The Journal has now highlighted three independent descriptions of 39 persons with a newly described syndrome characterized by thrombosis and thrombocytopenia that developed 5 to 24 days after initial vaccination with ChAdOx1 nCoV-19 (AstraZeneca), a recombinant chimpanzee adenoviral vector encoding the spike protein of SARS-CoV-2.3-5 These persons were healthy or in medically stable condition, and very few were known to have had previous thrombosis or a preexisting prothrombotic condition. Most of the patients included in these reports were women younger than 50 years of age, some of whom were receiving estrogen-replacement therapy or oral contraceptives. A remarkably high percentage of the patients had thromboses at unusual sites — specifically, cerebral venous sinus thrombosis or thrombosis in the portal, splanchnic, or hepatic veins. Other patients presented with deep venous thrombi, pulmonary emboli, or acute arterial thromboses. The median platelet counts at diagnosis were approximately 20,000 to 30,000 per cubic millimeter (range, approximately 10,000 to 110,000), but the rate of decline in platelet counts that preceded thrombosis is unknown. High levels of d-dimers and low levels of fibrinogen were common and suggest systemic activation of coagulation. Approximately 40% of the patients died, some from ischemic brain injury, superimposed hemorrhage, or both conditions, often after anticoagulation.
…
No thrombotic signal was detected in clinical trials leading to the approval of the ChAdOx1 nCoV-19 vaccine,9 which has now been administered to 34 million people worldwide. The incidence of VITT, as initially estimated, is perhaps 1 case per 100,000 exposures. This should be considered in the context of the incidence of cerebral venous sinus thrombosis in the general population (estimated at 0.22 to 1.57 cases per 100,000 per year).
https://www.nejm.org/doi/full/10.1056/NEJMe2106315
This is nice /sarc. It’s not been peer reviewed yet.
There is strong evidence for brain-related pathologies in COVID-19, some of which could be a consequence of viral neurotropism. The vast majority of brain imaging studies so far have focused on qualitative, gross pathology of moderate to severe cases, often carried out on hospitalised patients. It remains unknown however whether the impact of COVID-19 can be detected in milder cases, in a quantitative and automated manner, and whether this can reveal a possible mechanism for the spread of the disease. UK Biobank scanned over 40,000 participants before the start of the COVID-19 pandemic, making it possible to invite back in 2021 hundreds of previously-imaged participants for a second imaging visit. Here, we studied the effects of the disease in the brain using multimodal data from 782 participants from the UK Biobank COVID-19 re-imaging study, with 394 participants having tested positive for SARS-CoV-2 infection between their two scans. We used structural and functional brain scans from before and after infection, to compare longitudinal brain changes between these 394 COVID-19 patients and 388 controls who were matched for age, sex, ethnicity and interval between scans. We identified significant effects of COVID-19 in the brain with a loss of grey matter in the left parahippocampal gyrus, the left lateral orbitofrontal cortex and the left insula.
https://www.medrxiv.org/content/10.1101/2021.06.11.21258690v1
E.M. I think you saw this.
https://www.bitchute.com/video/aWXalrBhYAck/
Best short summary ;
“In order to get a patent on something it has to be “invented” and not natural. For example you can’t get a patent on “Vitamin C”. So, as this video reveals, almost all of the “components” of COVID19 have been patented (virus capsule, spike protein, furin cleavage site, etc). So, if this were a natural recombination occurrence, how did the bats and pangolins get the patented components? The video also reveals a lot of inconsistencies in the patent data, like PCR tests and vaccine patents being filed before the patents on the “novel” virus, etc.”
Any thoughts ?
The thing that keeps rattling in my brain is the Chinese Doctor that reported at the end of 2019 on his teams treatments of the first victims of this disease. It first appeared in young Chinese Army people that had been vaccinated with .a new SARs – Corona vaccine. He said that they sickened and died quickly, and there was little that they could do that worked for them. Massive doses of vitamin “C” was the first thing that they tried that worked for those that got secondary infections from the first ones. A couple Weeks later he was arrested and both he and his Internet report were “Disappeared”. The story that the virus appeared in the “Wet Market” caused by Bats, appeared, also the CCP floated the Meme that the virus was an American infection seeded from American troops that had attended a Military Olympics held in the late Summer.
@David A,
Well, there is no chemical man can make that the rest of nature can’t; and vice-versa.
Some doctors in my state have recently publicly stated that IV does not work. I don’t believe them. It is like they ignore data from other countries and in the U.S. also. Merck, the original maker of IV, is working on their new, expensive covid pill. Money, money and lies. People have to do their own research.